Embryo Hatching – Assisted IVF Technique Advantages and Risks
Assisted embryo hatching is a procedure based on the idea that artificially tearing the embryo`s shell, a zona pellucida, can increase the chances of implantation. In this post, we will explain the main advantages of assisted hatching, as well as possible risks.

The IVF protocol (in vitro fertilization) is a complex multistage process. Its success depends on many factors, and doctors still can’t control some of them. Even though the first child conceived with the help of IVF was first born back in 1978, no one guarantees the live birth after the first attempt. According to statistics, the first IVF round is successful in 30-50% of cases. And yet, thanks to new technologies, the percentage of pregnancies resulting from IVF is constantly growing.
Here is an example. Sometimes it is difficult for a human embryo to leave a so-called zona pellucida – a shiny transparent glycoprotein shell. Embryologists have found a solution. In this case, they use assisted embryo hatching, which helps the embryo free itself from the extracellular coat and implant into the uterus.
When Does an Embryo Normally Hatch?
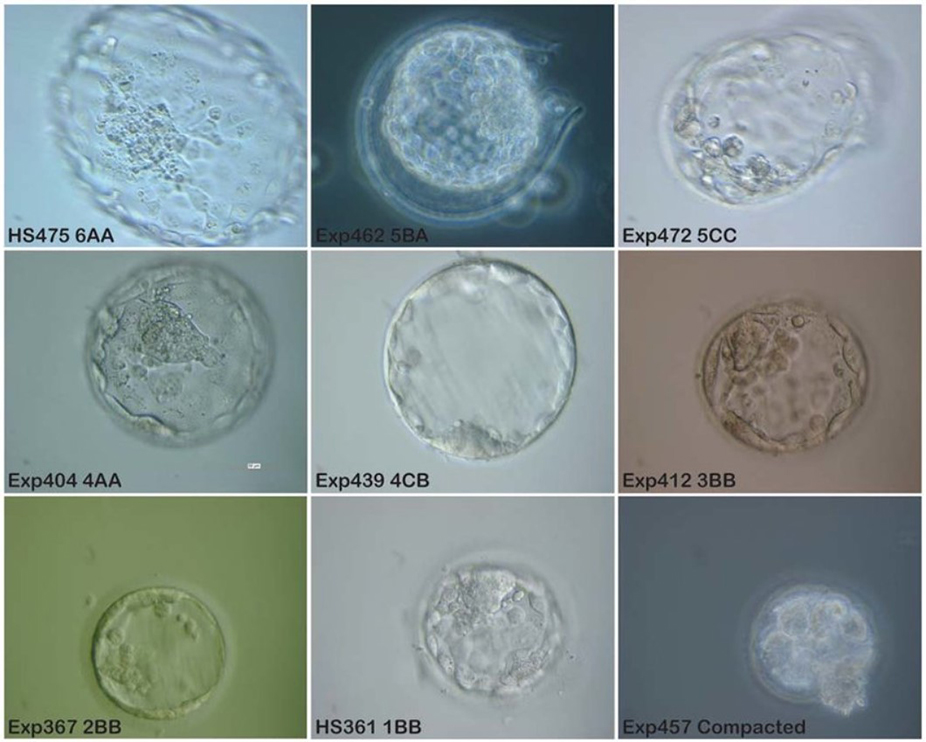
During the embryological stage in the clinic, the embryo goes through several phases during cultivation in the incubator. It grows from the oocyte on the day of puncture, through the zygote the next day, the stage of blastomere cleavage on days 2-3 of cultivation, morula on day four, and to the expected blastocyst on day 5.
And at all these stages, the embryo is reliably protected from external influences by the zona pellucida – a protein structure formed during maturation in the follicle. This membrane performs two proven functions – it provides a sperm block, that is, it does not allow more than one sperm to enter the egg and keeps the blastomeres next to each other at the cleavage stage. On the 5-7th day, the embryo reaches a large size, the zona pellucida becomes thinner and tears – the embryo hatches.
However, the embryo ruptures the zona pellucida not just because of its size; it releases lytic enzymes to break down the membrane proteins. Ideally, this is the case. It often happens that the embryo cannot break through the hard shell and remains in it – implantation does not occur. The question arises – maybe it is necessary to help it get out? The question remains controversial.
Why Do Embryos Need Assisted Hatching?
The inability of the embryo to attach to the wall of the uterus is one of the most common causes of female infertility. Embryo hatching is a natural process preceding implantation into the uterine cavity, during which the growing blastocyst is released from its membrane. Suppose natural hatching is difficult (often due to the thickening or hardening of the coat). In that case, assisted hatching comes to the rescue.
Assisted hatching is a microsurgical procedure successfully practiced with the most modern centers or clinics of reproductive medicine. The essence of the process is as follows. Before transferring the embryo into the uterine cavity, embryologists make a hole in its shell under a microscope or deliberately thin it out. It makes it easier to rupture the pellucid zone at the right time and significantly increases the chances of pregnancy. However, assisted hatching of the embryo is only used in special cases for medical reasons and is not part of the mandatory IVF program.
Indications for Assisted Embryo Hatching
As with any other medical procedure, assisted embryo hatching should only be performed on the recommendation of a specialist. It is not a panacea. More than that, in some cases, it may not affect the likelihood of pregnancy and is even harmful in some situations. But quite often, patients for whom assisted hatching is necessary for the onset of pregnancy ask doctors to use it during the IVF protocol. In what situations do doctors most often resort to assisted hatching? The list of indications looks like this:
- Maternal age is over 38 years old.
- The expectant mother is/was smoking.
- Impossibility of natural hatching.
- Exceeding the norm of follicle-stimulating hormone (FSH) follitropin in the blood.
- Low morphological parameters (unsatisfactory quality) of embryos.
- Thickening or other abnormalities of the pellucid zone.
- Transfer of cryo-frozen embryos.
- Several previous failed IVF attempts.
Why Are These Factors Important?
An increased basal level of follicle-stimulating hormone has a very negative effect on the effectiveness of assisted reproductive technologies. The percentage of pregnancies that have occurred decreases significantly even when the FGS level exceeds 15 mMU/ml on the third day of the cycle. Such indicators always entail the need for the use of technology.
An increase in the density of the pellucid zone is most often associated with the mature age of the expectant mother. Still, sometimes the reason for this is long-term measures to stimulate ovulation. The indication for assisted hatching is the embryo’s shell with a density higher than 18 nm. By the way, it is because of this compaction of the shell, that auxiliary hatching is usually prescribed after cryo-freezing of embryos.
As for the quality of embryos, their shape, cleavage rate, the presence or absence of nuclear-free fragments are of great importance – everything that can affect implantation in the uterus after transfer. If the embryos are not of the highest class III or IV and their fragmentation exceeds 10%, and if there are less than six blastomeres (cells formed at the initial stages of cleavage), then auxiliary hatching is also assigned.
4 Methods for Assisted Embryo Hatching
As for the methods by which assisted hatching is carried out today, dissection or thinning of the pellucid zone can be done in one of four ways.
Mechanical Embryo Hatching
The first of these is mechanical, which has been practiced since 1990. A special microneedle is inserted at an angle into the embryo’s shell not to damage its tissues. The resulting puncture facilitates the exit of the embryo from the pellucid zone.
Chemical
The second way is chemical. It is also time-tested – doctors have been using it since 1991. In this case, using a micropipette on the embryo membrane, choosing the safest zones, Tyrode’s acidic enzymatic solution is applied. After it makes a hole with a diameter of about 25 microns in the pellucid zone, doctors wash off the substance to avoid the negative effects of the chemical.
Piezo Technique
The third method of assisted hatching is the piezo technique. In this case, doctors fixate the embryo with a special micropipette, and apply a piezoelectric micromanipulator to its shell. Conical depressions in the pellucid zone result from high-frequency micro-vibration, contributing to the embryo’s early exit.
Lazer
The laser method has also been practiced for over 25 years and is considered the safest and most effective. In this case, the embryo’s shell becomes thinner without contact, using the most delicate narrow laser beam.
Assistive Embryo Hatching FAQ

Within the natural cycle, the hatching and implantation happen almost at the same time. Hatching usually happens on the 6th day after fertilization. It means, that if the doctors transfer an embryo that is already 5 days old, it will take 1-2 days to hatch. Starting from the 7th day, it is already possible to detect the hCG hormone in the blood.
You can use the word “embryo” to relate to any stage of the fetus’s development before its birth or hatching. The multi-celled embryo prior to hatching is called a blastocyst.
A hatching embryo looks like a round liquid sack filled with several cells and containing fluid inside it, with an outer shell, which tears during the hatching.
Assisted egg hatching is highly recommended for all FET (frozen embryo transfer) protocols. Unfortunately, not all embryos can survive thawing, therefore, it is highly important to give the remaining ones more chances to implant and help them hatch.
These assisted hatching methods have proven to be effective and safe for both the mother and the unborn baby. The patient chooses the most suitable one based on a thorough examination and subsequent recommendations of the reproductologist and embryologist. If you would like to know more about it, and check if you need to use assisted hatching for your IVF program – consult Sunshine fertility experts, we are always here to help.